Newsletter 3:2012
August 1, 2012
Continuing the topic of death with a functioning graft from the last CTS newsletter (May
2012), we would like to present new results that we find very impressive. We analyzed the
relationship between HLA matching and death with a functioning graft in deceased donor
kidney transplants performed during 1990-2010. The analysis revealed a striking and highly
significant relationship between donor-recipient HLA compatibility and mortality. Moreover,
the association between HLA compatibility and death varied according to whether patients
died from infection, cardiovascular death or cancer.
Figure 1 shows the most frequent causes of death reported to the CTS during the first three
years after kidney transplantation. These were infection (27%), cardiovascular disease
(30%) and, far less frequently, cancer (8%).
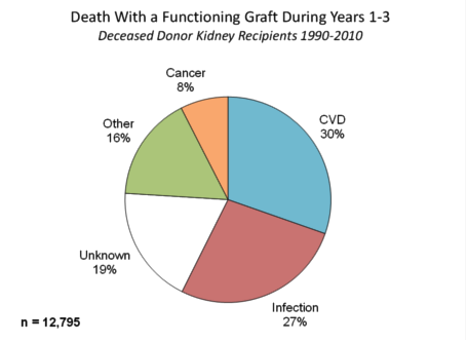
Figure 1
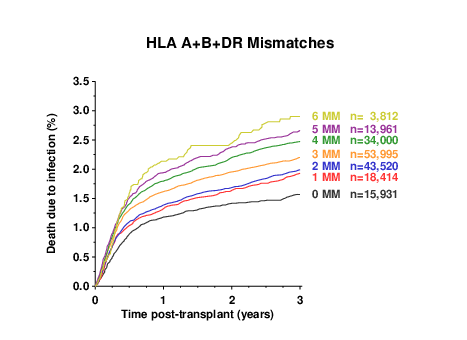
Figure 2
Figure 2 illustrates the association between matching for HLA-A+B+DR antigens and death
from infection. It shows an impressive graded relationship between the number of HLA
mismatches and infection-related mortality.
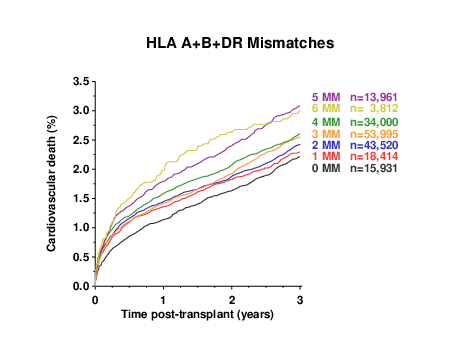
Figure 3
Cardiovascular death showed a similar, although slightly less strong, relationship with
HLA mismatching (Figure 3). Death from cancer, on the other hand, showed no relationship
whatsoever with the degree of HLA mismatch (Figure 4).
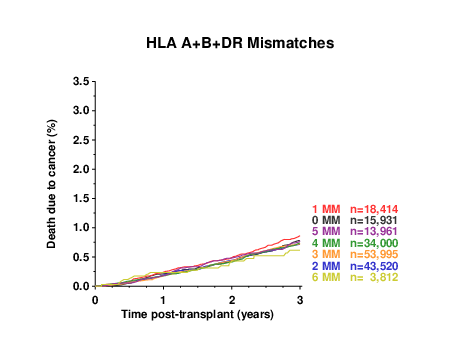
Figure 4
The association between death from infection and the number of HLA mismatches is most
plausibly explained by the need for stronger immunosuppression in patients who receive a
poorly matched kidney. A previous CTS study showing that the proportion of patients
requiring rejection treatment was directly proportional to the number of HLA mismatches
suggested that the extent of HLA mismatching determines the strength of the anti-graft
immune response (Transplantation 84:137-143, 2007). The consequent risk of overimmunosuppression
may result in fatal severe infection.
The close association between cardiovascular death and the number of HLA mismatches is
more difficult to explain, but may also be related to the stronger anti-graft immune response
and the requirement for more intense immunosuppressive treatment.
In view of these data on death from infection and cardiovascular death, the total lack of any
effect of HLA compatibility on death from cancer is somewhat unexpected, but not too
astounding since the progression of tumors is affected by many factors and HLA is clearly not
a strong factor.
Death with a functioning graft should now be added to the growing list of adverse
consequences for patients receiving a poorly matched kidney graft.
Many of us have just returned from the international TTS congress and are still digesting the wealth of information and
impressions we absorbed in Berlin. The congress was a vivid demonstration of the strength of both scientific and clinical
research in the field of transplantation. Even if the role of the CTS is small in this wider context, we are proud that,
in partnership with so many of you, we can broaden the knowledge base and contribute to the further improvement of results
in organ transplantation.
Thank you for your support!
Best wishes,
Gerhard Opelz