Newsletter 3:2013
August 1, 2013
In this issue of the newsletter, we would like to give you an update on the first 10 years of the
CTS Prospective Steroid Withdrawal Study. Although not randomized, the study is the largest prospective
steroid-withdrawal study ever conducted. Recipients of a kidney or heart transplant were enrolled
between 1994 and 2002. All patients received at least six months of post-transplant steroid treatment.
Steroids were subsequently withdrawn in patients who met the inclusion criteria, which selected
patients who had generally done well following transplantation. Outcomes in the steroid-withdrawal
patient group were compared to those of matched controls selected from the CTS database who
received maintenance steroid therapy. Three control patients were matched to each study patient
for a number of factors in order to minimize the likelihood of selection error. The first report
from the study, based on up to seven years of follow-up, was published in 2005 (Am J Transplant
2005; 5: 720-8) and describes the methodology in full.
The 10-year data are of great interest in view of concerns that steroid-free patients may experience
more long-term rejection and inferior graft failure rates versus those who continue steroid treatment.
Figure 1 shows the key results in recipients of kidney transplants from deceased donors: patient,
all-cause graft and death-censored graft survival rates after steroid withdrawal. It is evident
that patients in whom steroids were withdrawn showed an advantage compared to steroid-continuation
patients primarily in terms of patient survival. This observation supports the recent CTS finding
that death with a functioning graft due to infection or cardiovascular disease is associated with
the dosage of maintenance steroids (Association between steroid dosage and death with a functioning
graft after kidney transplantation. Am J Transplant 2013 [in press, doi: 10.1111/ajt.12313]).
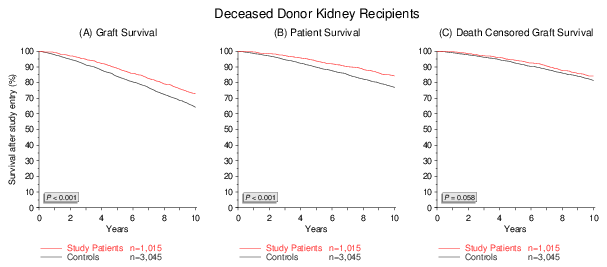
Figure 1
In heart transplantation, it is not necessary to analyze graft and patient survival separately because
graft and patient survival rates are virtually identical. With the rare exception of recipients who
are retransplanted, patients whose heart transplant fails die. The 10-year survival analysis is shown
in Figure 2. As seen in kidney transplants, heart transplant recipients in whom steroids were
discontinued had a superior 10-year survival rate as compared to controls who continued to receive
steroids.
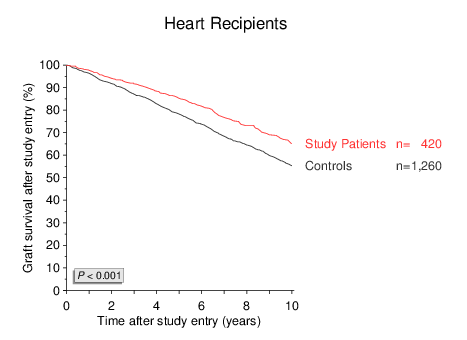
Figure 2
Data on treatment for rejection, kidney function and the incidence of osteoporosis and cataracts were
available in the subset of patients for whom the "CTS Extended Follow Up Questionnaire" was completed.
Kidney and heart recipients in whom steroids were withdrawn showed similar rates of treated rejections
to the matched steroid-treated control patients (Figure 3).
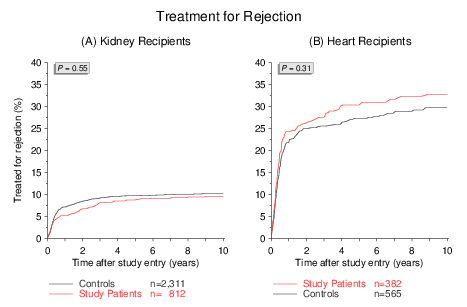
Figure 3
The only outcome measure for which a disadvantageous trend was observed in the steroid withdrawal group
was the rate at which serum creatinine level increased to >130µmol/L in kidney transplant recipients.
There was a small but significant increase in the proportion of recipients with impaired creatinine
among the steroid-withdrawal cohort (Figure 4A). When the analysis was repeated based only for patients
for whom it was known that they were indeed steroid-free during the entire observation period, this
group showed a significantly lower likelihood of poor kidney function than patients who required
steroids at any time during follow up (Figure 4B).
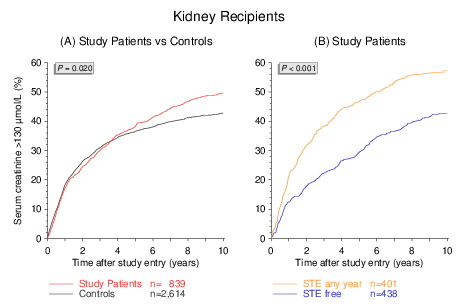
Figure 4
The incidence of osteoporosis and cataracts in steroid-discontinuation patients and controls is
illustrated in Figures 5A and 5B.
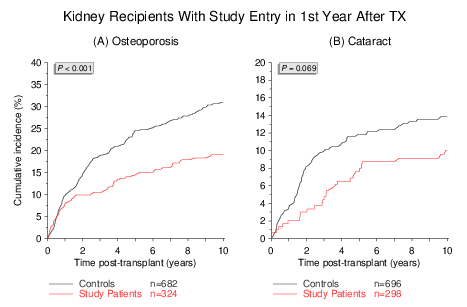
Figure 5
An advantage for the steroid withdrawal group was evident only in patients in whom steroids were
withdrawn during the first post-transplant year. For patients in whom steroids were withdrawn after
the first year, there was no effect on the long-term rates of osteoporosis or cataract versus
controls (data not shown), indicating that the damage inflicted by steroids regarding osteoporosis
and cataracts is inflicted relatively early and cannot easily be reversed.
In summary, this 10-year analysis confirms the earlier results from the study published in 2005.
It is reassuring that even 10 years after steroid discontinuation, immunosuppressive efficacy was
not compromised. Together with the recent observation that the dosage of maintenance steroids is
associated with cardiovascular death and death due to infection, evidence is mounting that patients
with adequate graft outcome benefit from a reduction in steroid dose or complete discontinuation
of steroids.
We would like to extend our special thanks to the centers that supported this CTS project by enrolling
patients in the CTS Prospective Steroid Withdrawal Study and providing long-term follow up data:
Kidney transplants: Banska-Bystrica, Barcelona, Belo Horizonte, Botucatu, Buenos-Aires, Cardiff,
Cologne-Merheim, Freiburg, Halle, Heidelberg, Izmir, Jena, Ljubljana, Mannheim, Marburg, Munich,
Newcastle (AUS), Nottingham, Oviedo, Pato Branco, Perth, Portland, Prague, Quebec, Santander,
St. Gallen, Szeged, Tours, Ulm, Valencia, Zurich
Heart transplants: Aalst, Bratislava, Edmonton, Essen, Kaiserslautern, Lausanne, London (Canada),
Melbourne, Montreal, Paris-Broussais, Perth, Prague, Sydney, Vancouver, Vilnius, Zurich
The next shipping date for the CTS serum and DNA studies is November 18/19, 2013. Thank you for your
consideration.
As always, thank you all for your continued participation in the international transplant study.
With best wishes,
Gerhard Opelz