Newsletter 4:2013
November 1, 2013
We recently reported an association between the daily dose of maintenance steroids and the
risk of cardiovascular death and death from infection in kidney transplant patients (Am J
Transplant 2013, 13:2096-2105). For this newsletter, we attempted to study the effect of
steroid dose in recipients of other types of organ transplant but encountered technical
problems. The proportion of liver transplant recipients receiving a higher dose of steroids
was too small for meaningful analysis. In heart and lung transplant recipients, the endpoint
cardiovascular death was not easily distinguishable from graft failure. However, analyzing
"death with a functioning graft due to infection" yielded very interesting results.
Figure 1 shows the rate of "death due to infection" according to steroid dosage at one year
after heart transplantation. During the period from year 1 to year 5 post-transplant, death
from infection showed a significant association with the daily dose of steroids.
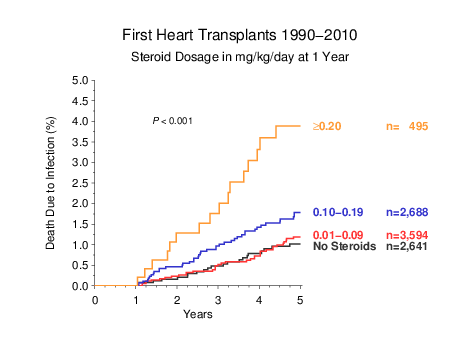
Figure 1
Of course, this result would not be very impressive if the patients who received higher doses
of steroids were those treated for rejection during the first post-transplant year. Therefore, we
looked specifically at patients who did not require high-dose steroid treatment for rejection
during the first year after transplantation. These patients showed an equally clear correlation
between daily steroid dosage at one year with death due to infection during years 2 to 5
(Figure 2).
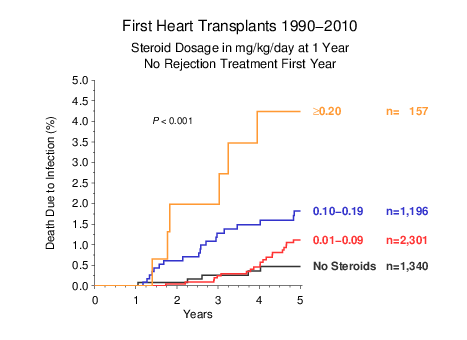
Figure 2
Applying even stricter criteria, we limited the analysis to patients who were not treated for
rejection and whose clinical outcome at one year was judged by the transplant center as
"excellent". Again, the association between maintenance steroid dose and death due to
infection was observed (Figure 3).
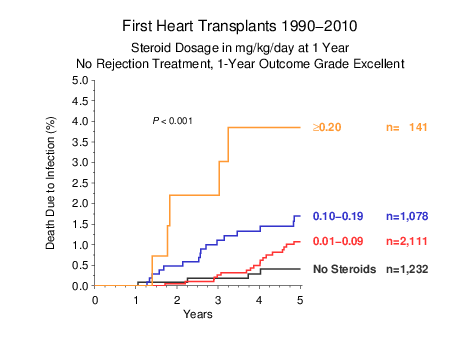
Figure 3
The results of an analysis in lung and heart-lung transplants were equally striking. Only
very few patients were receiving completely steroid-free maintenance immunosuppression at
one year. As in the heart transplant population, increasing steroid dose was strikingly
associated with death due to infection (Figure 4).
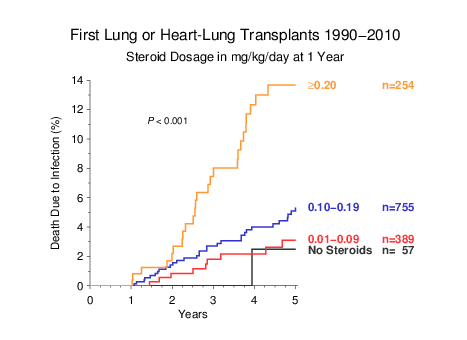
Figure 4
When the analysis was limited to those patients who were not treated for rejection during
the first post-transplant year, the association remained highly significant (Figure 5).
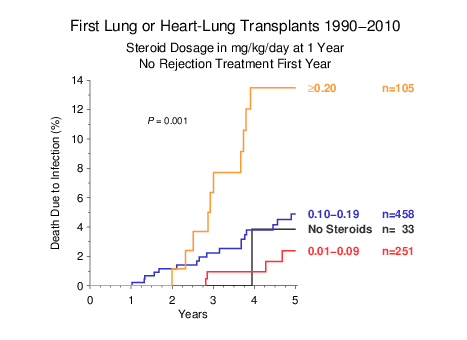
Figure 5
These results suggest that the association of maintenance steroid dose with death due to
infection applies to recipients of heart and lung transplants as well as kidney transplants.
According to these data, it would be beneficial to restrict high-dose steroid treatment to
patients for whom there is a definite clinical need. Since retrospective registry data have the
limitation that the rationale for administration of a given steroid dose is not documented, one
must, however, take a cautious approach. Carefully designed and well-documented
prospective studies would appear merited, to provide a conclusive answer.
If you have not yet returned your "Cancer Confirmation Questionnaire" for 2013, please check and
confirm the cancer data now. We can include your center in the CTS cancer analysis only if the questionnaire is returned.
Thank you for your support and cooperation!
Gerhard Opelz