Newsletter 3:2014
August 15, 2014
The CTS Newsletter 2:2000, which has been accessed on the internet more than 38,000 times,
addressed the topic of improving transplant success rates over the years, a trend that has
been updated recently in Transplantation 2013: 95; 4-7. Graft survival curves show that the
improvement in results was more impressive in earlier years, and has decreased to a
relatively slow pace more recently. In fact, it is surprising that there is any continuing
improvement at all, in the face of a parallel trend that we would expect to produce
lower success rates, i.e. the steady increase in the age of transplant recipients
and donors. Age is by far the single most influential factor affecting transplant
outcome. The evolution of recipient and donor age as reported to CTS for first
deceased donor kidney transplants is illustrated in Figures 1A and B.
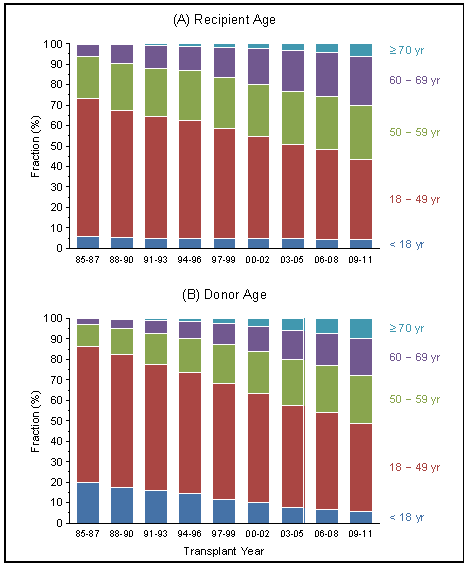
Figure 1
For this newsletter, we have prepared an analysis of risk for graft loss during successive
time periods, firstly based on the observed overall graft survival rates, and secondly
considering age, the dominating risk factor, as a confounder in a Cox model. The risk
for each interval is expressed as the hazard ratio (HR) based on the reference period
1985-1987 which was set at HR=1.00. First kidney grafts from deceased donors were analyzed.
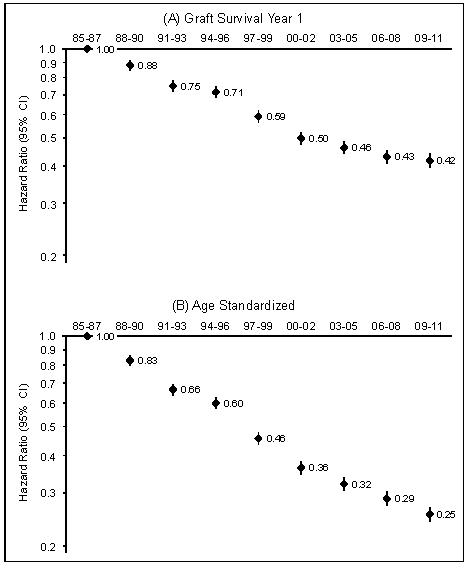
Figure 2
Figure 2A shows that the risk of graft failure - without considering recipient and donor
age - decreased stepwise from HR=1.00 for transplants performed in 1985-1987 to HR=0.42 for
transplants performed in 2009-2011. In other words, compared to the 1985-1987 reference
period, transplants performed 2009-2011 were less than half (42%) as likely to fail
within the first post-transplant year. When recipient and donor age are considered,
however, the risk of failure decreases even further from 1985-1987 to 2009-2011,
with HR=0.25 (Figure 2B). This result shows graphically what we all have suspected
for some time, namely that without the shift towards older recipient and donor age,
and the associated increase in age-related risk factors, the graft survival rate after
kidney transplantation would have improved even more impressively in recent years. Only
one out of four grafts transplanted during 1985-1987 that failed during the first
post-transplant year would have failed during the 2009-2011 interval had the distribution
of recipient and donor age remained unchanged.
Even more impressive is the change in patient survival over time, with or without the
confounder of recipient and donor age. Overall, the likelihood of death during the first
post-transplant year has decreased from HR=1.00 in 1985-1987 to HR=0.59 in 2009-2011
(Figure 3A). Taking into account that the average age of recipients and donors has
increased substantially over the years, the age-standardized analysis shows that a
transplant population in 2009-2011 would have had only a 25% risk of dying compared
to the patients transplanted in 1985-1987 if the age distribution had stayed the same
(Figure 3B).
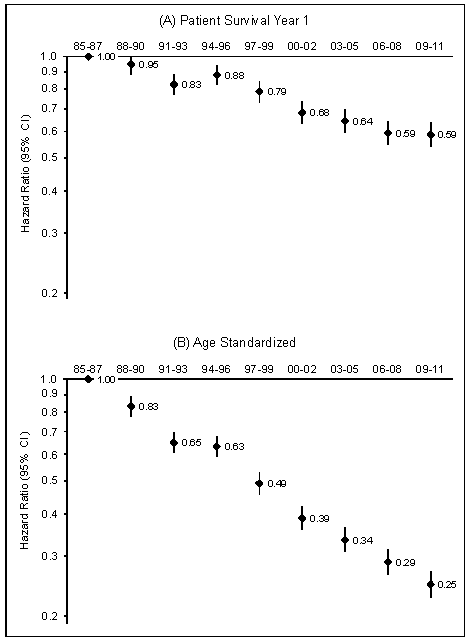
Figure 3
The results show similar trends for post-transplant years 2-5. Without considering
recipient and donor age, the risk of graft failure decreased from HR=1.00 for transplants
performed in 1985-1987 to HR=0.51 for transplants performed in 2006-2008 (Figure 4A).
With the consideration of age included as a confounder, the risk declined to just
HR=0.37 (Figure 4B).
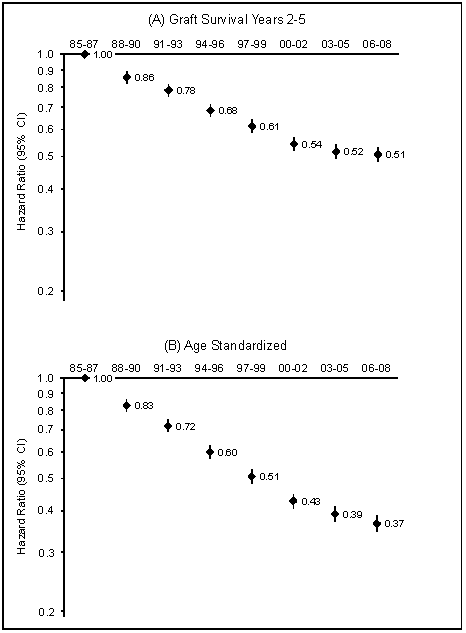
Figure 4
In the analysis of patient survival, the risk of dying during post-transplant years 2-5
decreased from HR=1.00 for patients transplanted in 1985-1987 to HR=0.67 for patients
transplanted in 2006-2008 (Figure 5A). When the fact that the recipient and donor age has
increased over time is taken into account, the age-standardized risk of dying during
post-transplant years 2-5 declines even more impressively, from HR=1.00 in 1985-1987
to HR=0.36 in 2006-2008 (Figure 5B).
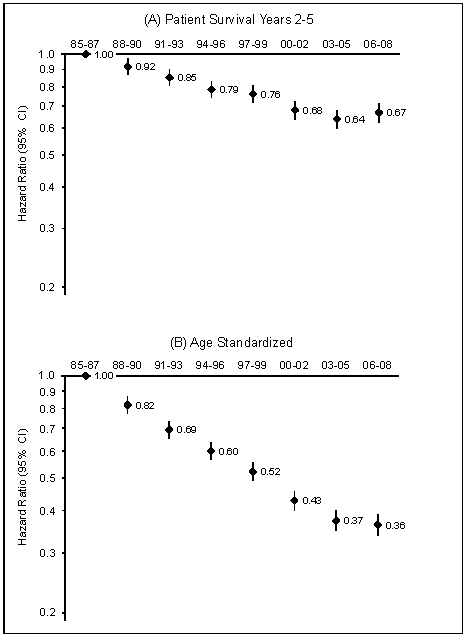
Figure 5
Unfortunately, age is not a modifiable factor. The evolution of population age has
affected the general non-transplant population as well as the transplant recipient
and donor populations. We are observing progressively higher means and medians for
recipient and donor age, a fact that we have to accept and which has, inevitably,
affected transplant outcomes. The overall improvement in observed patient and graft
survival rates means that other factors must have more than counterbalanced the
deleterious influence of higher recipient and donor age. Most probably, factors
such as improvements in immunosuppression, improved diagnosis and treatment of
rejection, better control of hypertension and hypercholesteremia, improved
prophylaxis, diagnosis and treatment of infection, and many other factors have
played a role. In all likelihood, greater experience by transplant professionals
and improvements in personnel training, as well as the availability of better
infrastructure in general have also contributed to the improvement.
Thank you as always for your continued support of the Collaborative Transplant Study.
Gerhard Opelz