Figure 1
CTS Collaborative Transplant Study
Dear Colleague
It is an often asked question why recipients of living donor kidney transplants generally enjoy better
graft survival rates than recipients of deceased donor organs.
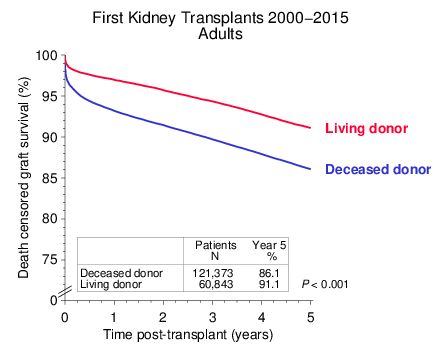
Figure 1
Death-censored survival rates of more than 180,000 first kidney grafts from living and deceased donors that were transplanted during the period 2000 2015 and reported to CTS are shown in Figure 1. Pediatric patients (≤ 17 years) and recipients of combined organ transplants were excluded. To illustrate short as well as long term effects, five-year outcome is depicted. The five year cut-off was chosen due to incomplete follow up for many patients after year five. Aside from factors relating to the general condition of the recipients, poorer organ quality, less favorable histocompatibility and increased immunogenicity of organs obtained after brain death may serve as possible explanations for the observed inferior outcome of transplants from deceased donors. We found it of interest to analyze the impact of donor-specific risk factors in greater detail.
Donor-specific factors that play an important role in deceased donor kidney transplantation are:
The individual influence of these factors on graft survival is demonstrated in Figure 2. Hereby the other risk factors were standardized (A: donor without hypertension and donor age < 50 years and ischemia ≤ 18 hours; B: donor death CVAS and donor age 50 64 years and ischemia = 18 hours; C: donor death trauma and donor without hypertension and donor age < 50 years; D: donor death CVAS and donor without hypertension and ischemia ≤ 18 hours). The impact of all four factors individually was statistically significant (P < 0.001).
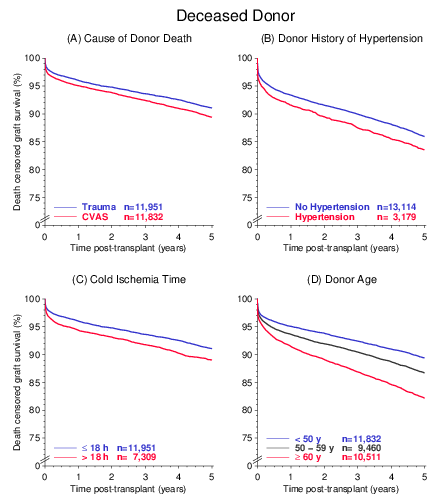
Figure 2
Among the four risk factors, high donor age has the strongest negative impact on outcome. Currently, approximately one-third of the deceased donor organs originate from ≥ 60 year old donors. Additional analyses demonstrated that the influence of donor age is less pronounced in living donor kidney transplantation and furthermore that the presence of two risk factors is associated with worse outcome than the presence of just one risk factor (not shown).
Importantly, as shown in Figure 3A, the absence of all four of these risk factors in deceased donors (Good DD) may result in a virtually identical graft success rate as that seen with living donors (All LD). However, while this is true for transplantations performed in Europe, North America and Australia/New Zealand, it does not apply to other continents where kidneys from deceased donors continue to show an inferior outcome, even if the donors do not possess any of the described risk factors (Figure 3B). The reasons for this are in all likelihood multifactorial and not everywhere the same.
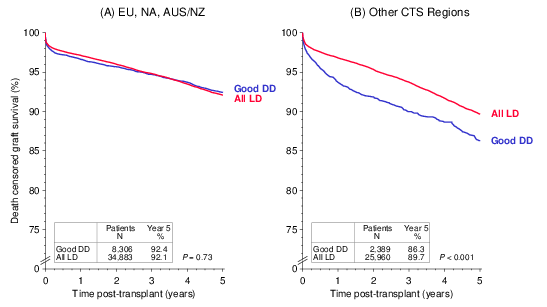
Figure 3
Another issue of interest is the impact of the HLA compatibility between donor and recipient. As shown in Figure 4, '0 HLA-A+B+DR mismatch' is a special category; recipients of these kidneys with excellent matches, whether from living or deceased donors, enjoy excellent graft survival in all regions of the world.
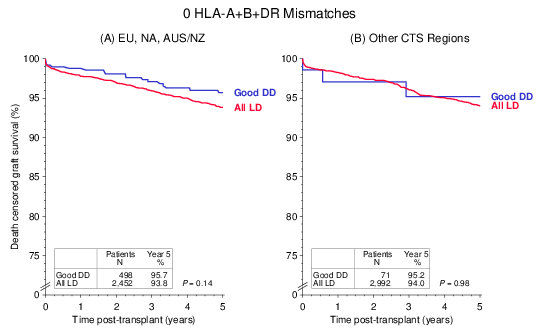
Figure 4
I would like to thank you very much for your continued trust and support. Please use the new CTS forms for data entry on which we request also the information on donor-specific antibodies. The early first results from this information already suggest that interesting new findings will be generated from these data. Do not hesitate to contact us if you have ideas for study subjects. Our capacity is limited but we will do our best to include your suggestions. Already, several interesting papers are being prepared based on ideas contributed by CTS participants during the last few months and we will soon share the results with you.
The next shipping date for the DNA and serum studies is June 19/20, 2017.
Yours sincerely,
![]()
Caner Süsal