Figure 1
CTS Collaborative Transplant Study
Dear Colleague
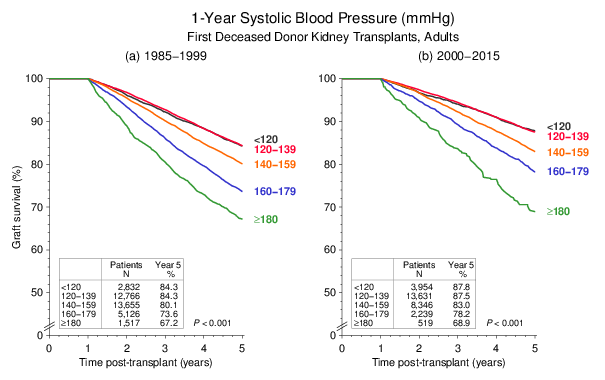
In the year 1998, CTS published on the striking influence of the systolic blood pressure
one year after transplantation on subsequent kidney graft survival
(Opelz G, Wujciak T, Ritz E. Association of chronic kidney graft failure with recipient blood
pressure. Kidney Int 53: 217222, 1998). Kidney transplants performed in the years
19871995 were analyzed for this paper. Whereas the overall graft survival rate has improved
significantly since that time, the effect of hypertension on graft outcome can be demonstrated
equally convincingly for kidney transplants performed during the recent 20002015 period
(Figure 1). It is also gratifying to see that the treatment of hypertension has improved.
As many as 61 % of recipients transplanted during 19851999 had a 1-year systolic blood pressure
of ≥ 140 mmHg, the corresponding figure for patients transplanted 20002015 was 43 %.
Figure 1
In stark contrast, no influence of blood pressure on graft survival can be shown in heart and liver transplant recipients (Figure 2). The proportion of patients with systolic blood pressure of ≥140 mmHg at year one was 42 % both in heart and liver recipients.
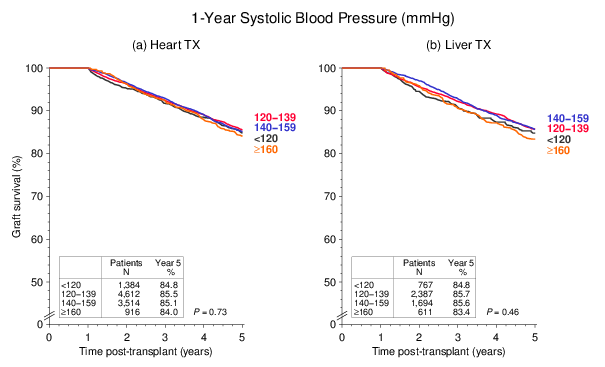
Figure 2
Chronic kidney disease is common after heart or liver transplantation, with calcineurin inhibitors (CNI) considered the key contributor. A possible influence of posttransplant blood pressure had not been extensively examined. In a CTS report by Morath et al, which will soon be published in the journal Transplantation, the 1-year blood pressure was identified as the dominant modifiable risk factor associated with deteriorating kidney function during the years two to five after heart or liver transplantation. It was found that for patients with a serum creatinine of <130 μmol/L at year one, deterioration of renal function increased with the level of blood pressure.
We would like to support and extend these findings here using a modified approach in which the analysis was not limited to patients with good renal function after one year. All patients in the current analysis had a functioning graft for at least five years and were transplanted before Oct 31, 2012. Creatinine values have been captured in the CTS in the four categories <130, 130260, 260400 and >400 μmol/L. Figure 3 shows the incidence of patients with increasing creatinine values from year one to five by at least one category. A striking correlation between one year blood pressure and decrease of renal function to year five is apparent both in heart and liver recipients.
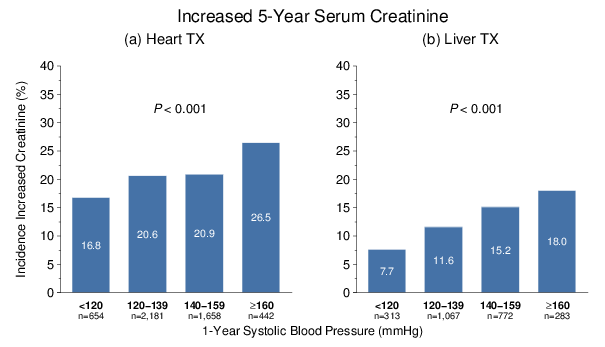
Figure 3
It is well known that blood pressure and serum creatinine generally rise with increasing patient age. This was taken into account by showing that the strong relationship between blood pressure and renal function can be demonstrated for younger as well as older patients (heart or liver recipients were combined in this analysis), taking 55 years of age as a cut-off (Figure 4).
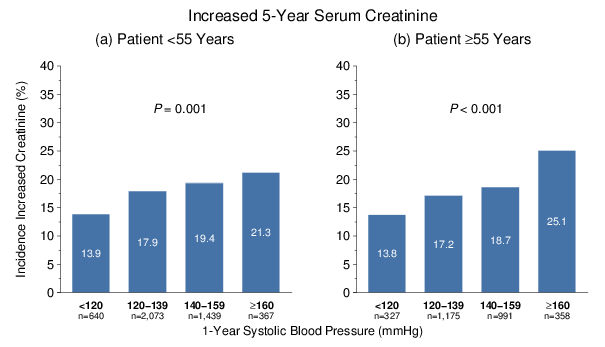
Figure 4
Although the treatment of hypertension has greatly improved over the years, Figure 5 shows that the deleterious influence of increased blood pressure on renal function is still clearly demonstrable in recent times.
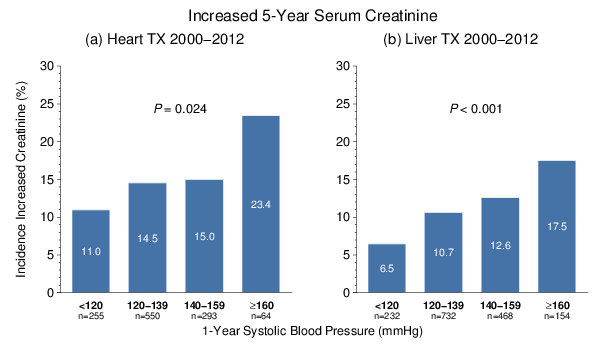
Figure 5
To our surprise, neither the type of CNI nor the CNI dose or trough level at year one showed a significant association with kidney function at year five. Figure 6 illustrates the influence of daily CNI dosage on renal function for heart and liver transplants since 1998 (low: cyclosporine <150 mg/day or tacrolimus <3.0 mg/day; high: cyclosporine >250 mg/day or tacrolimus >6.5 mg/day; according to interquartile ranges).
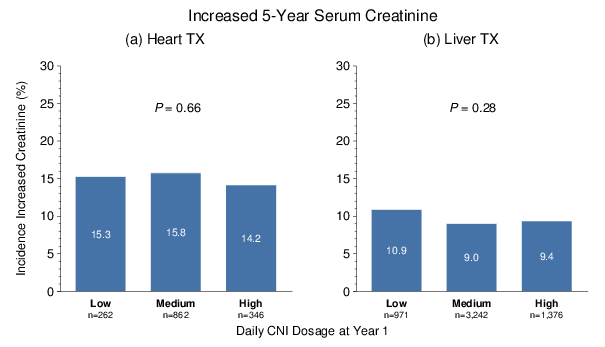
Figure 6
The 18th ESOT Congress took place in Barcelona from 24 to 27 September. An ESOT Young Investigator Award went to:
Maarten
Coemans, Leuven, Belgium
OS265 - SHORT AND LONG TERM GRAFT SURVIVAL AFTER KIDNEY TRANSPLANTATION IN EUROPE
Authors:
Maarten Coemans1, Caner Süsal2, Geert Verbeke3,
Maarten Naesens1
Affiliations:
Department of Microbiology and Immunology, University of Leuven1,
University of Heidelberg2, Leuven Biostatistics and Statistical
Bioinformatics Centre3
This oral presentation was the result of a successful cooperation between CTS and participating centers. Do not hesitate to contact us if you have ideas for research projects with CTS data.
The next shipping date for the DNA and serum studies is November 13/14, 2017.
Thank you very much for your continued support of the CTS.
Sincerely yours,
![]()
Caner Süsal