Figure 1
CTS Collaborative Transplant Study
Dear Colleague
In 2009, we reported in the journal Transplantation on the impact of early adverse events in kidney transplantation and their association with preformed HLA antibodies (87: 13671371). The analysis comprised 1,134 deceased donor kidney transplants on which, in addition to a pre-transplant serum, detailed information on clinical events during the early post-transplant period was obtained within the CTS Pre-Transplant Serum Study. More than twice as many patients have been recruited in the meantime in this special CTS sub-study. The much higher number of 2,951 patients with a longer follow-up now allows an in-depth analysis of these events and their influence on graft and patient survival. We concentrated on two adverse events, namely delayed graft function defined as no graft function during the first 24 h (DGF) and acute rejection episodes during the first 3 post-transplant months (ARE).
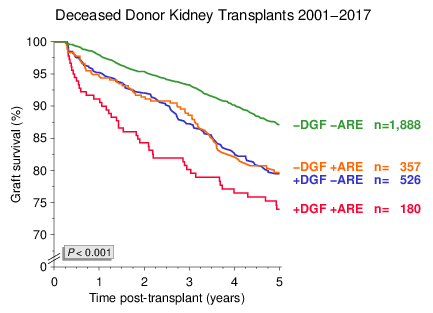
As illustrated in Figure 1, the individual impact of DGF and ARE on 5-year graft survival from month 3 was similarly strong and independent of each other. If the early adverse events occurred simultaneously (+DGF +ARE), their impact was impressive.
Figure 1
Because of the almost identical individual influence of both events, the group of patients without DGF and ARE (DGF/ARE) was compared in further analyses with the three small groups merged into one adverse event group (+DGF/ARE). Early adverse events had a significant impact on both death censored graft as well as patient survival (Figure 2). The influence on death censored graft survival was, however, more pronounced (hazard ratio 2.0 vs. 1.6).
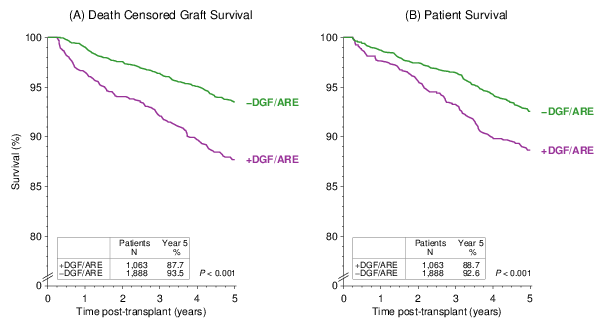
Figure 2
As demonstrated in Figure 3, early adverse events influenced not only short- but also long-term graft survival.
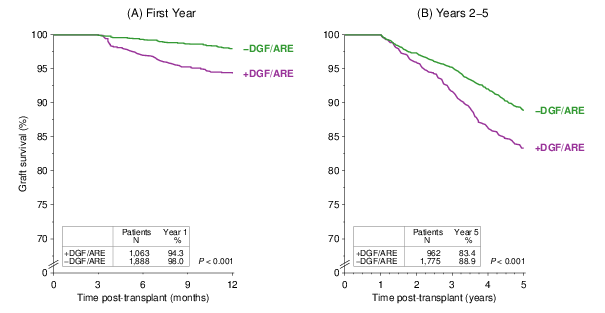
Figure 3
In the 2009 Transplantation paper we reported on a significant association of ARE as well as DGF with ELISA-reactive HLA antibodies that were present in the patients pre-transplant serum. The occurrence of early adverse events in patients with different HLA antibody constellations is illustrated in Figure 4. As compared to antibody-negative patients (I II), a higher incidence of early adverse events was observed in patients with only HLA class I (+I II), only HLA class II (I +II) or both HLA class I and class II antibodies (+I +II). In several previous publications we pointed out that the co-presence of ELISA-reactive HLA class I and class II antibodies is an important risk factor and patients with this antibody constellation should be transplanted under special precautions (Transplantation 73:12691273, 2002; Transplantation 90: 645653, 2010). As compared to antibody-negative patients (I II), both adverse events together occurred at an almost 3-fold higher rate in class I and class II antibody-positive patients (+I +II). As was already shown in Figure 1, the simultaneous occurrence of DGF and ARE had a striking impact on subsequent outcome.
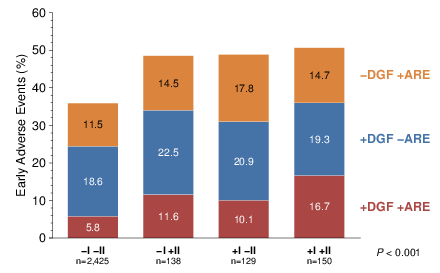
Figure 4
Comparison of patients with and without adverse events in the early post-transplant period revealed differences also in known confounders of graft survival. Significantly older donors (median 53 y vs. 47 y, P<0.001), a longer cold ischemia time (mean 17.6 h vs. 16.3 h, P<0.001) and more retransplants (16.1 % vs. 11.8 %, P<0.001) were noted among patients with early adverse events, whereas sex, recipient age, geographical region, transplant year and initial immunosuppression were not significantly different in the two groups. To consider the influence of these differences, we separated the study population into low risk (donor age 60 y, cold ischemia time ≤24 h, no ELISA-reactive HLA antibodies, first transplants) and increased risk patients (all others).
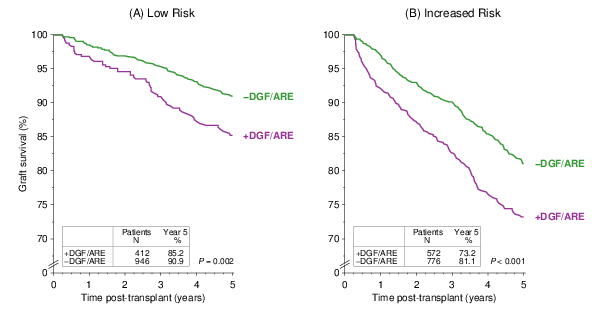
Figure 5
The early adverse events influenced graft survival not only in increased risk but also in low risk patients (Figure 5). As one would expect, increased risk patients showed an inferior outcome overall and the fraction of patients who experienced early adverse events was significantly higher in the increased risk than in the low risk population (42.6 % vs. 31.9 %, P<0.001).
These findings were confirmed in multivariable Cox-regression analysis in which the following confounders were considered: transplant year, geographical region, transplant number, recipient and donor age and sex, original disease, cold ischemia time, time on dialysis, HLA-A+B+DR-mismatches, ELISA-reactive HLA class I and II antibodies, induction therapy and immunosuppressive medication. A 62% higher risk of graft loss during the first 5 post-transplant years was found for patients with early adverse events (hazard ratio 1.62; 95% confidence interval 1.341.97; P<0.001). As compared to patients analyzed in the Transplantation paper in 2009, the fraction of patients with early adverse events has decreased somewhat despite an increasing donor age, from 38% during 20012007 to 34% since 2008. Remarkably, the hazard ratio for graft loss due to early adverse events has increased from 1.54 to 1.74.
Our results indicate that even in the era of sensitive HLA antibody screening techniques, the pre-transplant presence of ELISA-reactive HLA antibodies is a significant risk factor for the development of the early adverse events DGF and ARE. Preventive measures, early diagnosis and timely treatment of early adverse events might contribute to further improvements in kidney graft survival.
We are indebted to those of you who have been participating in the CTS Pre- and Post-Transplant Serum Studies. All findings presented in this Newsletter are based on this CTS special project. Please continue to send us material for these studies which reveal results with important clinical implications.
The next shipping date of Serum and DNA is
November 19/20.
Thank you very much for your trust!
Sincerely yours,
Caner Süsal