Figure 1
CTS Collaborative Transplant Study
Dear Colleague
During the last 20 years, we reported in several CTS publications on the striking impact of blood pressure on the renal function of organ transplant recipients:
· Opelz G, Wujciak T, Ritz E. Association of chronic kidney graft failure with recipient blood pressure. Collaborative Transplant Study. Kidney Int. 1998; 53: 217222.
· Opelz G, Döhler B. Improved long-term outcomes after renal transplantation associated with blood pressure control. Am J Transplant. 2005; 5: 27252731.
· Opelz G, Zeier M, Laux G, Morath C, Döhler B. No improvement of patient or graft survival in transplant recipients treated with ACEI or ARB. J Am Soc Nephrol. 2006; 17: 32573262.
· Morath C, Opelz G, Döhler B, Zeier M, Süsal C. Influence of blood pressure and calcineurin inhibitors on kidney function after heart or liver transplantation. Transplantation. 2018; 102: 845852.
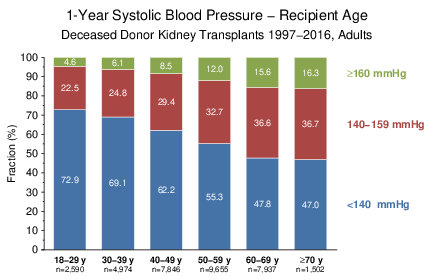
The well-known strong relationship between increasing patient age and elevated systolic blood pressure is illustrated in Figure 1. The systolic blood pressure one year after transplantation is shown for different age categories in ≥18-year-old recipients of deceased donor kidney grafts who were transplanted during 19972016. To ensure a homogeneous study population, the analysis was restricted to kidney-only transplantations from Europe, Australia/New Zealand, and North America. Despite antihypertensive medication, more than half of the ≥60-year-old recipients had an increased 1-year systolic blood pressure of ≥140 mmHg, the WHO's threshold for defining hypertension.
Figure 1
In addition, the proportion of ≥60-year-old recipients has been steadily increasing. Currently, more than one-third of deceased donor kidney transplant recipients belong to the age category ≥60 (Figure 2).
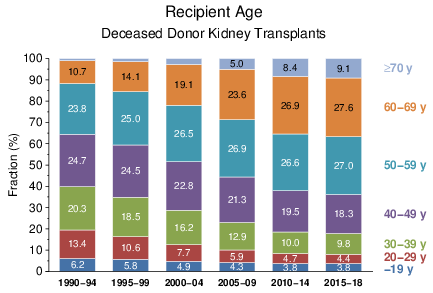
Figure 2
However, as compared to 18−59-year-old recipients, the influence of systolic blood pressure on graft survival is, although statistically significant, less pronounced in ≥60-year-old patients (Figure 3). This is also true for death-censored graft as well as patient survival (not shown).
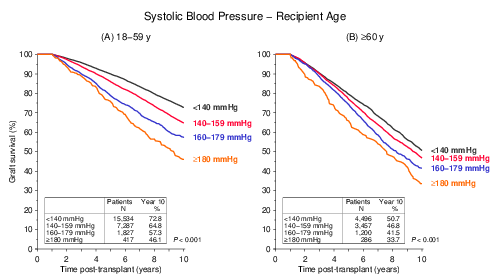
Figure 3
A further CTS publication on the impact of blood pressure entitled 'Pulse Pressure and Outcome in Kidney Transplantation' will soon appear in the journal 'Transplantation'. This time, we focused on 'pulse pressure', the difference between systolic and diastolic blood pressure. Especially interesting for us were the results obtained in elderly patients, in whom a decrease of diastolic blood pressure frequently leads to high pulse pressure.
In ≥60-year-old kidney recipients, besides high systolic pressure, an increased pulse pressure at year 1 post-transplant also had a significant impact on graft survival. The diastolic pressure was not influential. Underlining its independent effect, pulse pressure influenced graft survival also in elderly recipients with normal (Figure 4A) or mildly elevated (Figure 4B) systolic blood pressure. However, in elderly patients with normal systolic pressure only the patient survival was influenced by an increased pulse pressure; death-censored graft survival remained unaffected (Figure 6 of our Transplantation paper in press).
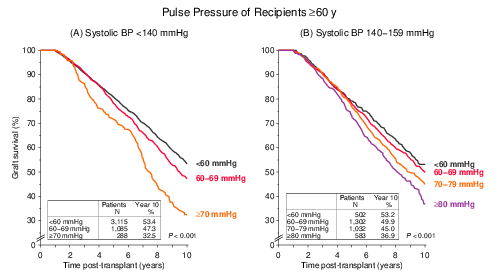
Figure 4
As shown in Figure 5, a pulse pressure of ≥60 mmHg at post-transplant year 1 significantly increased the mortality due to cardiovascular disease (CVD) in ≥60-year-old patients with a normal systolic blood pressure of <140 mmHg. Mortality due to infection or cancer was not influenced.
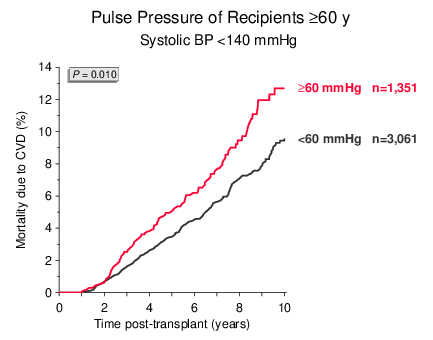
Figure 5
As shown in Figure 2, elderly patients are a steadily increasing population among deceased donor kidney transplant recipients. In this analysis, patients with a high pulse pressure made up almost one third of the ≥60-year-old patients with normal systolic blood pressure. In clinical routine, erroneously these patients might be categorized as normal-risk patients.
As every year in January, all outcome graphs on the CTS homepage have been updated. The new graphs can be accessed either using the CTS password attached to this newsletter or via your center-specific CTS account. You are welcome to use the CTS graphs in your presentations or teaching activities without special request. However, if you wish to include CTS graphs in your publications, please be so kind and read the CTS citation policy under the link http://www.ctstransplant.org/public/policy.shtml.
This is also the time for checking whether all transplants performed at your center during the year 2018 were reported to CTS. Please report any missing transplants as soon as possible.
The next shipping date of Serum and DNA is
June 17/18, 2019.
On behalf of the whole CTS-Team, I wish you a peaceful and healthy 2019!
Sincerely yours,

Caner Süsal