CTS Collaborative Transplant Study
Dear Colleague
In previous CTS newsletters and publications we repeatedly addressed the topic of continuously improving short- and long-term outcomes in deceased donor kidney transplantation (CTS Newsletters 2:2000 and 3:2014, the Transplantation paper by G. Opelz in 2013 [doi:10.1097/TP.0b013e3182754c88] and the Kidney International paper by M. Coemans et al. in 2018 [doi:10.1016/j.kint.2018.05.018]. In this newsletter we would like to inform you on the developments in living donor kidney transplantation.
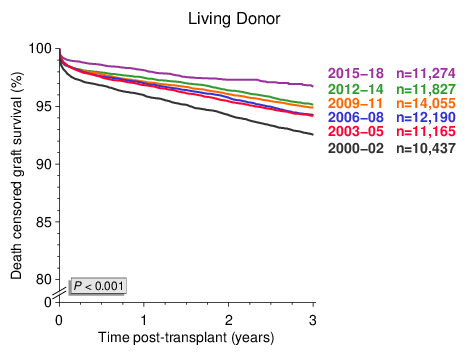
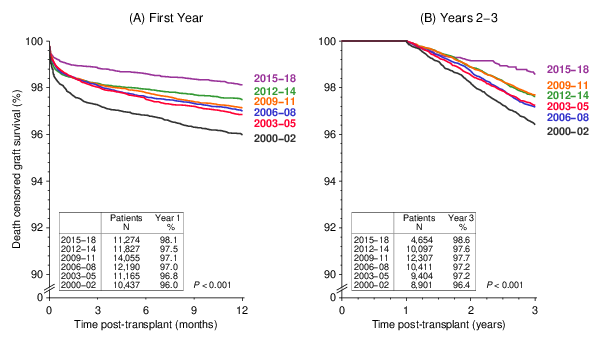
Also in recipients of living donor kidney transplants, death censored graft survival rates have been improving continuously since 2000 and an additional impressive improvement is now observable in transplantations performed during the most recent period 20152018 (Figure 1). As illustrated in Figure 2, this positive change is not restricted to the early phase after transplantation, it is evident also after the first post-transplant year.
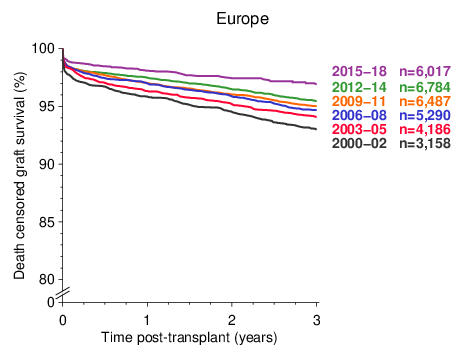
This CTS analysis includes results of living donor kidney transplantations from 335 transplant centers in 46 countries. The analyzed dataset might therefore be considered to be inhomogeneous due to center-based variation. In fact, the observed improvements were evident in all geographical regions. Figure 3 illustrates exemplarily the analysis for Europe.
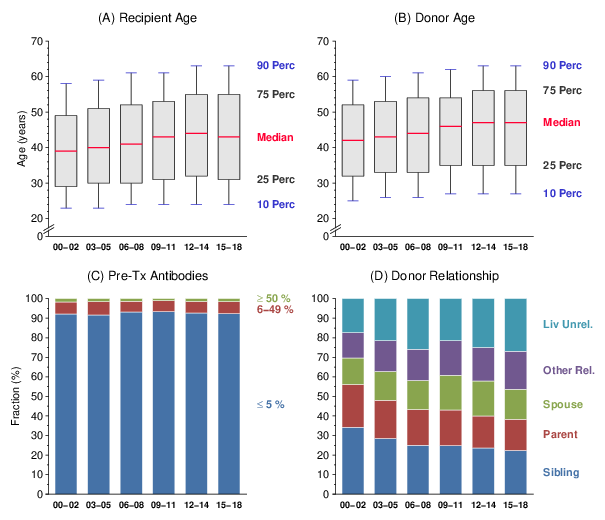
The evolution of recipient age (increase of median by 4 years), donor age (increase of median by 5 years), pre-transplant cytotoxic antibodies (no major change) and donor relationship (decrease in the parental and sibling transplantations) from 2000 to 2018 is demonstrated in Figure 4. Recipient age is a strong influential factor in living donor kidney transplantation. Therefore, the continuing improvement of graft survival despite this negative trend is impressive.
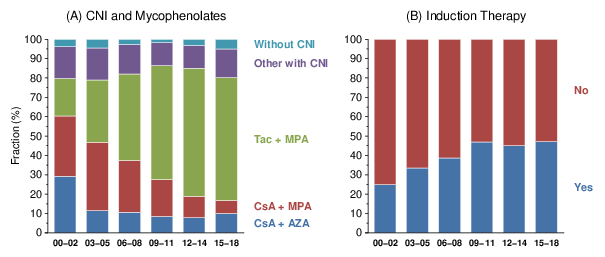
The immunosuppressive therapy has changed substantially during the analyzed period of 19 years. Meanwhile, for nearly two thirds of the patients, treatment with tacrolimus plus mycophenolates and for nearly half of the patients, induction therapy with antibodies became standard (Figure 5). Additional analyses, however, indicated that the changes in immunosuppression alone were not able to explain the observed developments; the most recent impressive improvement during 20152018 occurred under similar drug combinations as in the previous 20122014 period.
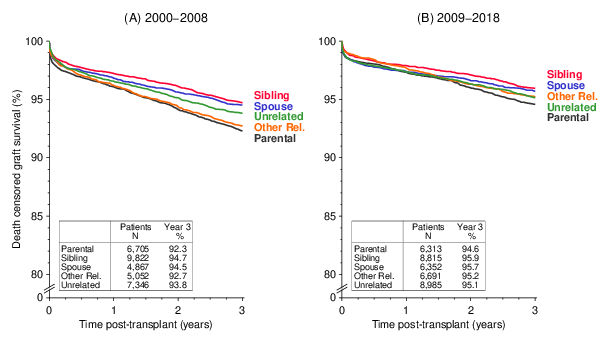
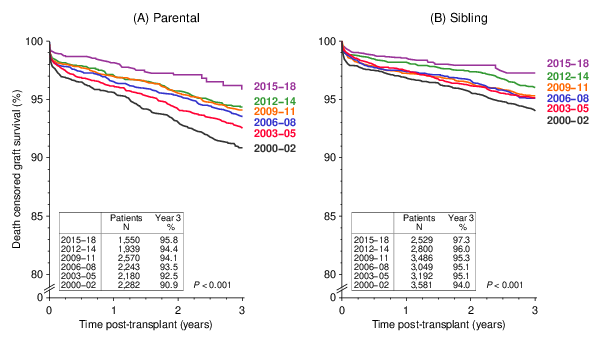
A further development that accompanied the overall improvement of graft survival rates was the influence of donor relationship which, as compared to the 2000-2008 period, has diminished during the more recent 20092018 period (Figure 6). The improvement was evident both in parental transplantations with the lowest as well as sibling transplantations with the best graft survival rates (Figure 7).
With the rather limited numbers of cases in the decisive subgroups, we can only speculate about the factors that are responsible for the still ongoing improvement of success rates. Sensitive alloantibody testing, better health condition of selected donors, effective antiviral prophylaxis, diagnosis and treatment, better control of hypertension, and improved infrastructure and patient management in concert are the possible explanations.
Please note that the presented results are based on most recent data and the follow-up is, as is to be expected, partly incomplete. Only with more complete follow-up will we be able to affirm the genuineness of these very pleasing developments. We will continue informing you.
If you have not been able to join the ongoing CTS Pre- and Post-Transplant Serum Studies, please consider your participation. These studies continue to reveal results with important clinical implications.
The next shipping date of Serum and DNA is
November 18/19, 2019.
Thank you very much for your continued support of the CTS.
Sincerely yours,

Caner Süsal